What Are the Challenges Facing Gender Equality in Tanzania?

Gender Equality
All women should have access to equal opportunity and the ability to exercise their rights, such as access to quality education, productive work, land ownership, and making informed decisions regarding their sexual and reproductive health. These are central components to gender equality and giving women the ability to live in the kind of safe environment they deserve. Women need to be free to make their own informed choices and have the same access to education, resources, and opportunities as their male peers. Empowered women in Tanzania continue to work towards enabling the next generation to have healthy and productive families and communities. But there is still a long way to go. The Afrobarometer Dispatch reported in 2017 that even though around 75% of Tanzanians feel the government is doing fairly well at promoting gender equality, there are still several major barriers for women in Tanzania to overcome.

These barriers are social norms that make it much harder for a woman in Tanzania to have the same freedoms, education, resources, and opportunities as men.
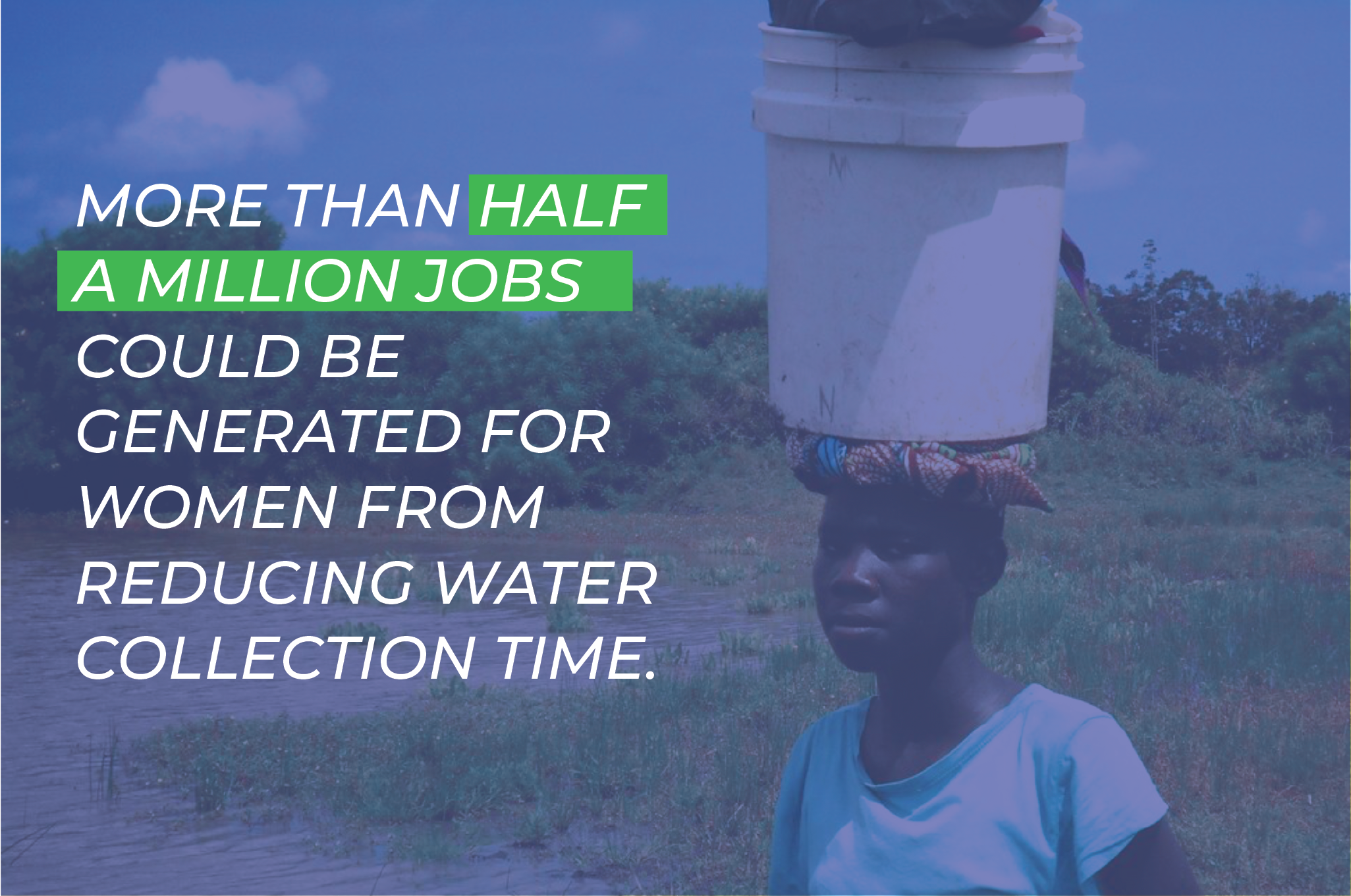
- Women lack time. Women spend more time on household chores than men. Not only are they the primary caregivers for children and in charge of running the household, they are also responsible for collecting water and firewood. Approximately 78% of women spend time collecting water daily, compared to only 33% of men. These tasks are not only unpaid, but are tiring, strenuous, and time-consuming, which leaves less time and fewer opportunities for women to have paid work to help make their family’s life better.
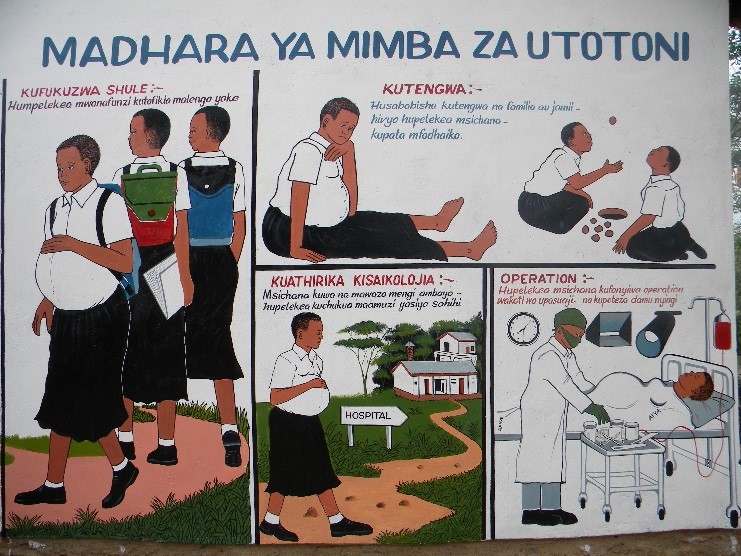
- Girls are less educated, resulting in fewer opportunities in the workforce. Even though primary level schools in Tanzania have achieved gender equality, and 80% of children attend school, many girls fall behind when they enter secondary level education (largely due to their menstrual cycle or early pregnancy). This results in women entering the workforce with less opportunity and lower levels of pay.
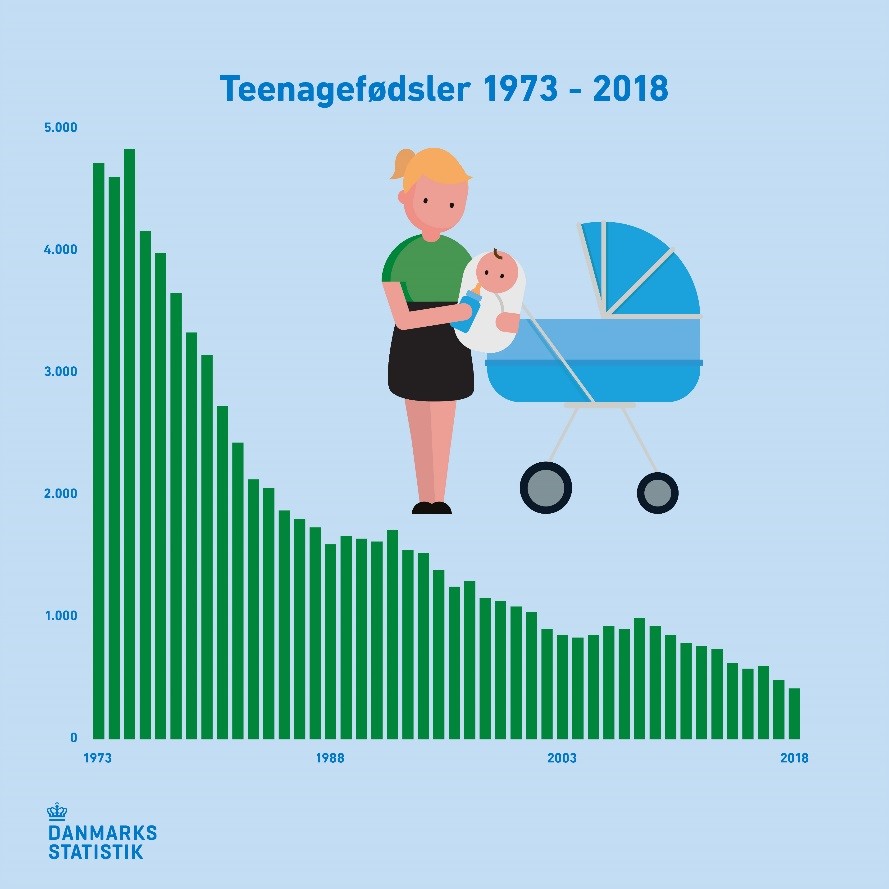
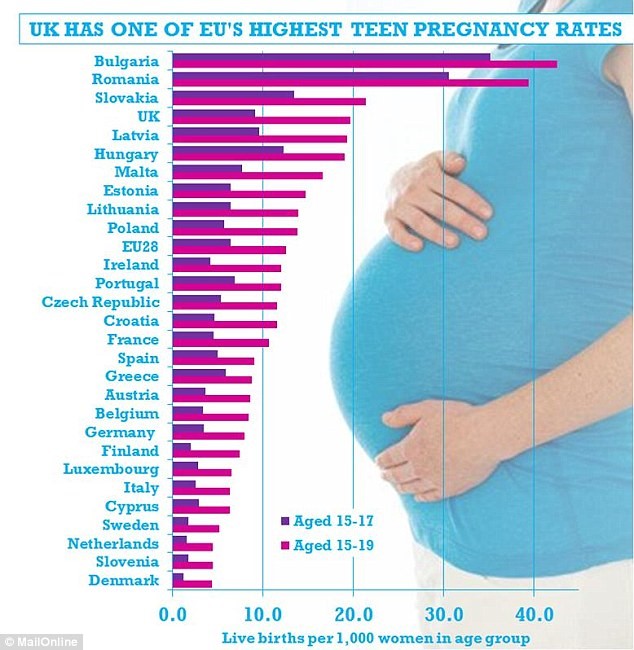
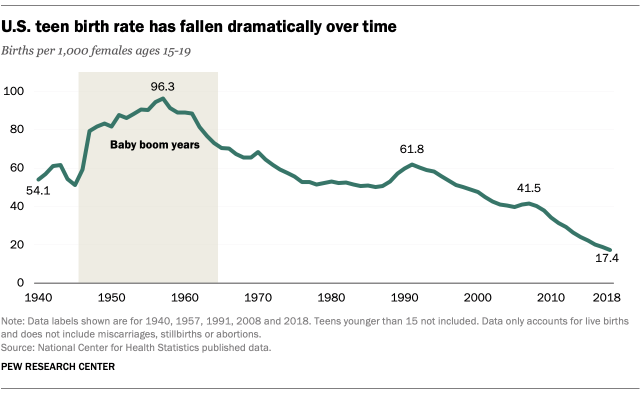
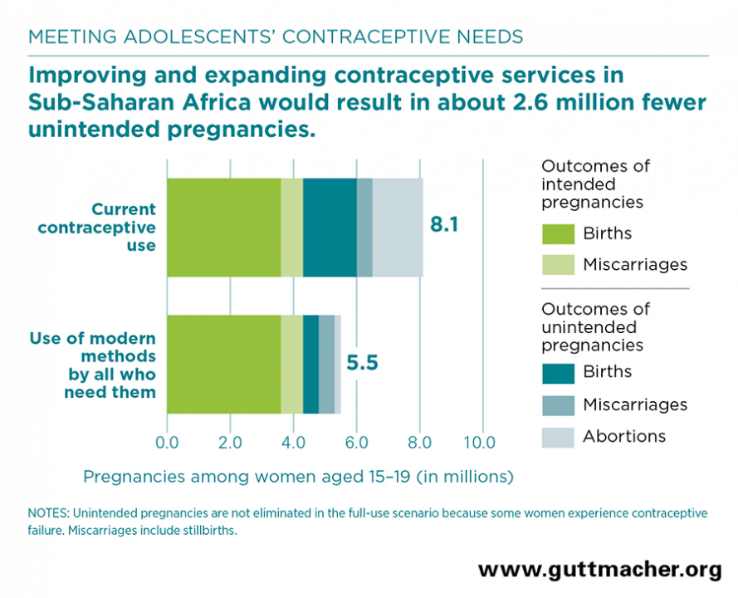
- Women lack freedom when it comes to reproductive health. With high early marriage and teenage pregnancy rates in Tanzania, education and employment opportunities are often taken away from women. Pregnant girls are typically kicked out of school and become the primary caregivers in their homes. Access to information about birth control is often attacked by those in power, thus reducing a woman’s ability to choose how many children she wants to have and when, where, and with whom she wants to build a family.

- Access to owning property, assets, and financial services is difficult to achieve. Because women have less education and fewer opportunities than their male peers, they often have smaller plots of land, own less livestock, and earn less income. It is also more likely that their land is for subsistence farming rather than making a profit. Most financial providers do not consider women a large target group, so they have less access to financial services. Most women have to start a business with their own savings because interest rates are too high for them.
Moving Forward towards Gender Equality
Despite the challenges women in Tanzania face, government improvements have been implemented, so more women can thrive and live a productive life that includes recreation and rest. If tasks, such as water and firewood collection and household chores, were shared with their male peers, or the time spent on chores was reduced with technology, huge amounts of time could be freed up for women to pursue employment and paid work. In fact, one study calculated that more than half a million jobs could be generated for women from reducing water collection time, about 225,000 from reducing fuel collection, and around 4 million from reducing time spent on food preparation.

Conclusion
While gender equality for women is something most Tanzanians support, there is still long way to go. Even though some progress has been made when it comes to removing the barriers women face, Tanzanian females still do not have equal rights and opportunities. MSG is committed to working towards changing this through our programs, so women have bright futures as leaders and change-makers. Our staff has always been over 75% women, and we are committed to helping other women and girls break the barriers they face when it comes to rights, opportunities, finances, owning property, and earning an income. Our programs specifically focus on menstrual hygiene health and women’s empowerment – factors that are changing the game for women in the areas where we work. We hope to continue to expand our work to reach more women and prevent these barriers from keeping them from reaching their full potential.
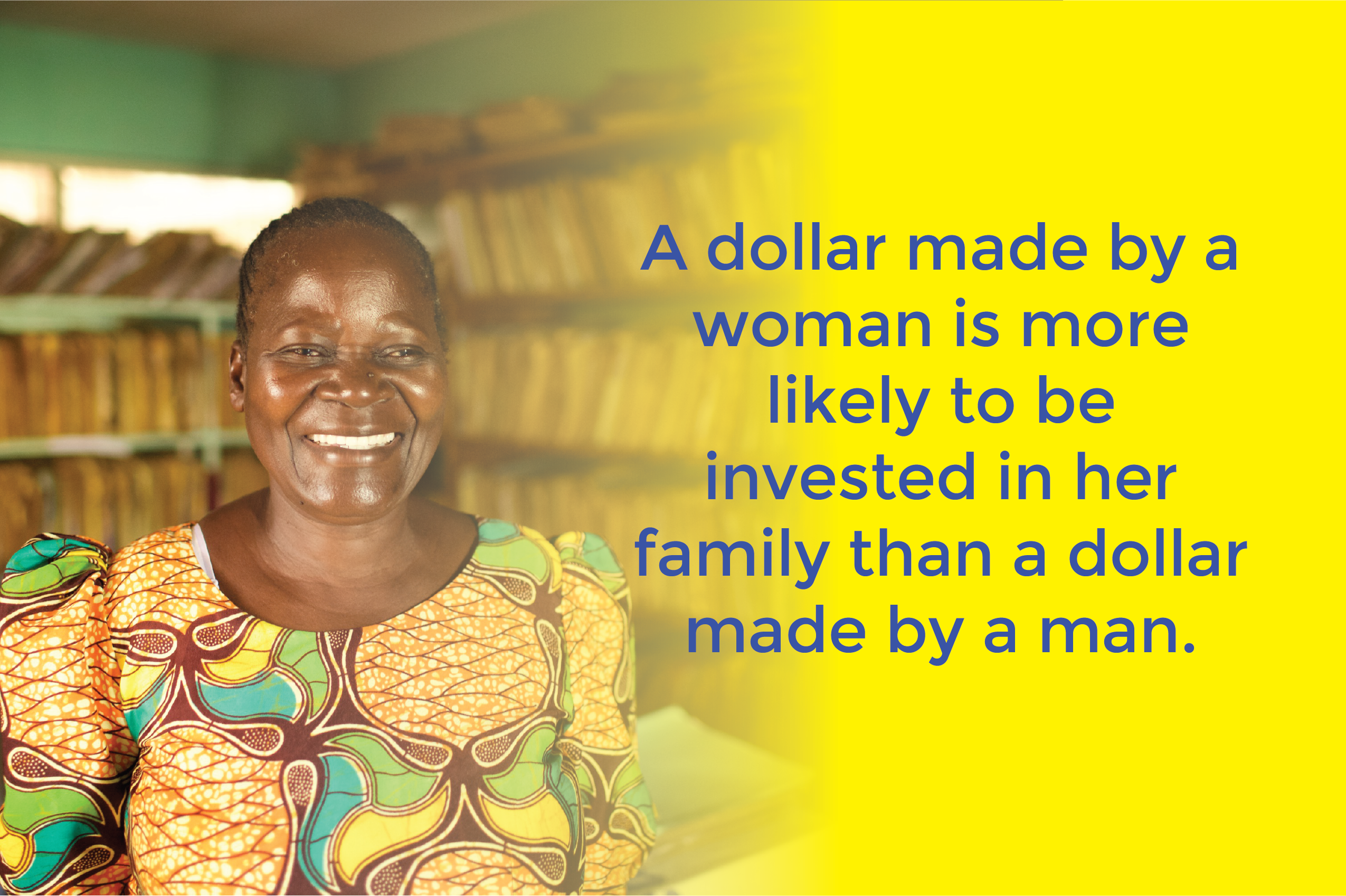
By empowering women we will also empower families!
Historical Context of Gender Inequality in Tanzania
Pre-colonial Era and Indigenous Systems
Pre-colonial Tanzania was characterized by a variety of governance structures, social norms, and economic systems, with some ethnic groups practicing matriarchal systems, and others patriarchal. Women’s roles and power varied greatly among these societies. In many communities, women were instrumental in agriculture, family care, and even held certain leadership roles.
Colonial Impacts on Gender Roles
However, the advent of colonialism brought significant shifts. Colonial rule, which spanned the late 19th to the mid-20th century, profoundly altered the social fabric. The period was marked by the imposition of foreign laws, education systems, and economic structures, all of which had lasting implications for gender dynamics. Colonial powers often reinforced patriarchal systems, sidelining women from decision-making processes and formal economic participation.
Post-independence Efforts and Shortcomings
Post-independence in the 1960s, Tanzania embarked on various nation-building and economic restructuring processes. The socialist policies under President Julius Nyerere recognized the role of women in nation-building. However, while these policies were progressive on paper, their implementation often fell short, failing to dismantle many of the deeply entrenched gender norms and economic barriers.
Modern Policies and Persistent Challenges
The late 20th and early 21st centuries have seen a more concerted effort to address gender disparities. Tanzania has ratified several international agreements aimed at promoting gender equality. Moreover, while there have been strides towards legal reforms to protect women’s rights, societal norms and practical realities often lag behind legal advancements.
Economic Impacts of Gender Inequality
Gender Disparities Stifling Economic Growth
Gender inequality isn’t just a social issue in Tanzania; it’s an economic challenge with far-reaching implications. The economic participation of women is crucial for sustainable development, poverty reduction, and the overall economic health of a nation. However, when women are not given equal opportunities to participate in the workforce or are limited to lower-paying jobs, the entire economy suffers. Studies indicate that gender inequality reduces a country’s economic growth and leads to lower GDP.
Women’s Unpaid Labor: The Invisible Contributor
One of the significant economic impacts of gender inequality is the undervaluation of women’s work. In Tanzania, women often bear the brunt of unpaid labor, such as childcare, eldercare, household chores, and subsistence farming. This work, though essential for the welfare of families and communities, is rarely accounted for in economic analyses and, therefore, remains invisible in GDP calculations. Recognizing, reducing, and redistributing unpaid work through shared household responsibilities and the provision of public services are critical steps towards improving women’s economic status.
Education and Workforce Participation
Educational disparities between genders in Tanzania lead to unequal workforce participation. With many girls receiving less education than boys, particularly at the secondary level, women enter the workforce with fewer skills and opportunities for formal employment. This not only affects individual women and their families but also limits the available talent and labor pool in the country, stymieing innovation and economic growth.
Land Ownership and Financial Inclusion
Access to economic assets is another area where the impacts of gender inequality are starkly visible. Women in Tanzania face legal and cultural barriers to owning land and accessing financial services, which hampers their ability to start or expand businesses. Improving women’s property rights and financial inclusion is not only a matter of fairness but also a prerequisite for the economic development of the country. When women can own land, they can secure loans, invest in their businesses, and contribute more significantly to the economy.
Gender Pay Gap: A Persistent Challenge
Even when women do participate in the formal economy, they often face a significant wage gap compared to men. This gender pay gap is due not only to direct discrimination but also to occupational segregation, with women overrepresented in lower-paying sectors and underrepresented in leadership positions. Closing this pay gap is essential for economic justice and for improving the overall economic health of the nation.
Macro-Economic Policies and Gender Budgeting
At the policy level, macro-economic strategies and budgeting processes often overlook the gendered impacts of fiscal decisions. Adopting a gender-responsive budgeting approach ensures that national economic policies and budgets are analyzed for their effects on gender equality and women’s empowerment, leading to more equitable outcomes.















 Computer-generated design of WASH Hub. So far, MSG has established a borehole and built a laundry block and an office building.
Computer-generated design of WASH Hub. So far, MSG has established a borehole and built a laundry block and an office building.  Together with MSG staff, the Ward Counselor officially opened the initial phase of our WASH Hub on March 7, 2023.
Together with MSG staff, the Ward Counselor officially opened the initial phase of our WASH Hub on March 7, 2023.









 My WASH career started in 1978 when I was hired as the first WASH-sector specialist for the Peace Corps. Throughout my career, infrastructure has always been the first thing people wanted to fund and the easiest. However, there are huge issues with the sustainability of projects, and they have yet to have any real impact. For real influence, you need to change people’s behaviors. In the 1980s, the new big thing was the ultimate hand pump designed by engineering schools with a technical mentality. Additionally, much more money has gone into disease treatment and drugs rather than prevention, which is much cheaper in the long run.
My WASH career started in 1978 when I was hired as the first WASH-sector specialist for the Peace Corps. Throughout my career, infrastructure has always been the first thing people wanted to fund and the easiest. However, there are huge issues with the sustainability of projects, and they have yet to have any real impact. For real influence, you need to change people’s behaviors. In the 1980s, the new big thing was the ultimate hand pump designed by engineering schools with a technical mentality. Additionally, much more money has gone into disease treatment and drugs rather than prevention, which is much cheaper in the long run. The first experience that interested me in WASH was carrying water as a Peace Corps volunteer in the 1960s at the school in Tanzania where I was teaching. After a few days, I hired a young man to fetch it for me and realized what a colossal problem water was. Later, while working in northern Kenya on a medical mission during my master’s work on the Turkana tribe, I also saw first-hand the impact of drought on people and the desperate need for clean and clear water.
The first experience that interested me in WASH was carrying water as a Peace Corps volunteer in the 1960s at the school in Tanzania where I was teaching. After a few days, I hired a young man to fetch it for me and realized what a colossal problem water was. Later, while working in northern Kenya on a medical mission during my master’s work on the Turkana tribe, I also saw first-hand the impact of drought on people and the desperate need for clean and clear water. Two of my proudest achievements have been helping start Friends of Tanzania 27 years ago, which has been worthwhile and successful, and representing the Peace Corps when the UN launched their Water Decade in 1980 because they were going to solve the problem by 1990. But unfortunately, that did not happen, and I have seen many examples of unmet goals like that. For example, the Carter Center was going to eliminate the guinea worm disease by 1990, then 1995, then 2000, but is still working on it because of the difficulty of changing people’s behaviors.
Two of my proudest achievements have been helping start Friends of Tanzania 27 years ago, which has been worthwhile and successful, and representing the Peace Corps when the UN launched their Water Decade in 1980 because they were going to solve the problem by 1990. But unfortunately, that did not happen, and I have seen many examples of unmet goals like that. For example, the Carter Center was going to eliminate the guinea worm disease by 1990, then 1995, then 2000, but is still working on it because of the difficulty of changing people’s behaviors.